
Are private practice Credentialled Diabetes Educators on the endangered list?
Jayne Lehmann BN(Ed) DipAppSc(Nsg RN CDE
The Medicare funded Chronic Disease Management program has provided reimbursement for people with diabetes to see a Credentialled Diabetes Educator (CDE) in primary care since 2004. Introduced as an eligible service in the Chronic Disease Management program, given the 1.4million people living with diabetes in Australia, you would expect the numbers of CDE sessions saw steady growth.
Well … that’s what you would think … but when I reviewed the Medicare data today, a very different trend was revealed.
Medicare data tracks the number of sessions delivered by CDEs in each state and territory, and I’ve been reviewing this data ever since I became a Medicare provider in 2004. I pulled off the latest figures today to review how diabetes education session numbers have been tracking in each state and territory up to June 2018. That’s 14 years of data and you would expect to have seen a steady increase in the number of sessions provided by CDEs over the years given we have so many people with diabetes in Australia and a relatively small number of CDEs in private practice.
Here’s the chart below … and I hope you can hear alarm bells sounding when you look at the chart.
See the steady growth in the number of services delivered each year in most states and territories from 2004 – 2011-12? Now look at the years after that and you will see a significant slowing in the numbers being referred to CDEs via this program.
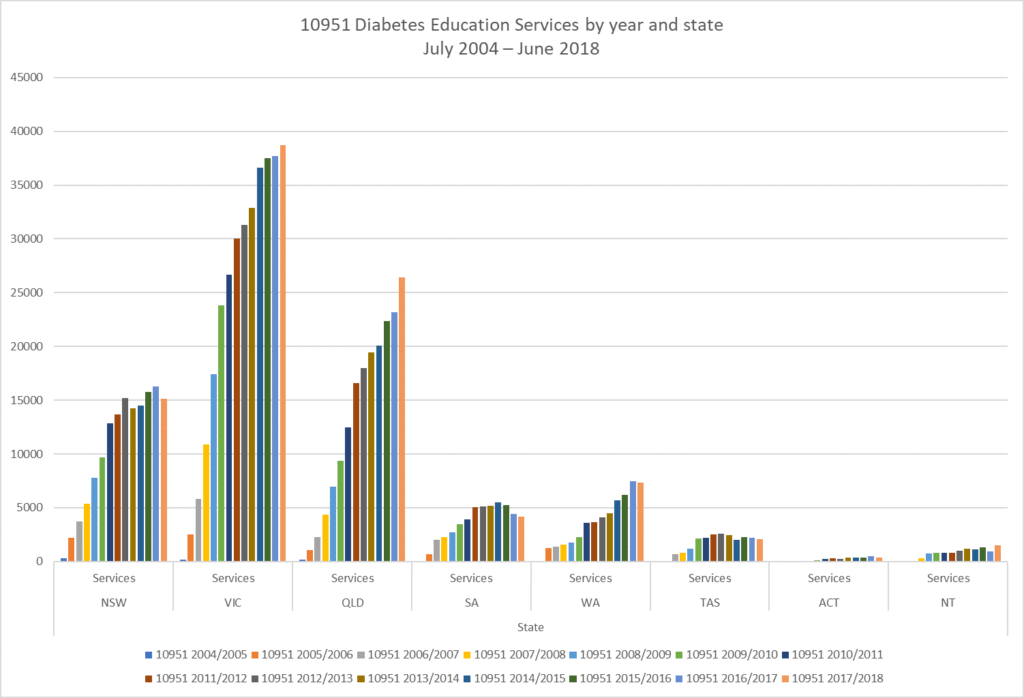
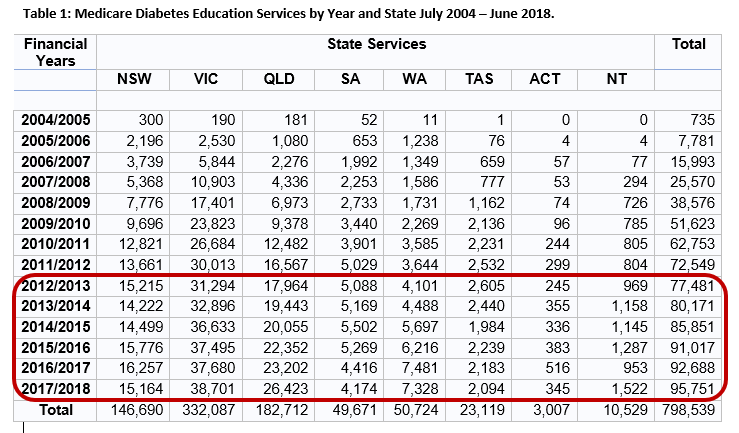
Chart 1: Medicare Diabetes Education Services by Year and State July 2004 – June 2018.
So why is this so?
2012 saw the freezing of Medicare rebates to all health professionals. Consequent income stream analysis within general practices saw them identifying new opportunities to access the primary care nursing item number for diabetes services. More nursing clinics were initiated to help pay for nursing services in primary care and offset the decreasing Medicare income by GPs. After all, the practice costs continue to rise even if the Medicare levy doesn’t.
The Medicare freeze in 2012 also impacted he income of CDEs, as their reimbursement was frozen at the same time. This was not lifted until a few days ago, on 1st July 2019, a year after GPs. CDEs in private practice have identified a decrease in their income from the rebate freeze and at the same time there has been a noticeable trend for the majority of general practitioners not to refer people with diabetes to CDEs in private practice. The number of sessions people are referred for has also decreased, often to one appointment. I, and many others, have had to increase my fee for those without a disability and those who are not financially stressed. Even so, I do end up bulk billing the majority of people I see and once you take into account the cost of the systems, my time, those who do not turn-up and having to spend more time with people because of the low number of sessions allocated per referral, I estimate my hourly wage to be $5 per hour for bulk billed diabetes education services. This is essentially an unsustainable downward pressure on wages for CDEs in private practice.
With all of this this in mind, look at the session numbers from 2012-13 to June 2018 in the table below. The growth in diabetes education sessions via Medicare significantly slowed across Australia, with five states and territories experiencing negative growth in at least one financial year in that time. The other two states (Victoria and Queensland) had their lowest growth of 185 sessions (2015 – 16 and 2016 – 2017) and 622 sessions (2013-14 – 2014 – 2015) respectively, in the data up to June 2018.
In order to understand this drop in Medicare reimbursed CDE services you need to recall that the Royal Australian College of General Practitioner’s Diabetes Management Guidelines made a significant change in their recommendations to GPs (and the broader audience of health professionals who read and utilise these guidelines) about blood glucose monitoring for people with type 2 diabetes in 2014. The literature reviewed for the Guidelines identified that people with type 2 diabetes not prescribed insulin gained little, or no, benefit from blood glucose monitoring. It is unfortunate the review did not take into account the work by William Polonsky and Larry Fisher on structured blood glucose monitoring, which has shown a benefit because it included strategies to inform people of the appropriate times to check their levels, what the numbers mean and how they could act on the numbers to have them sit in the target range for longer.
Soon after, the Commonwealth Government announced restricted access to blood glucose monitoring strips for people with type 2 diabetes not prescribed insulin. When you add to these two events the increased distribution of blood glucose meters by nurses in general practice and community pharmacy, you start to understand the decreased referrals by GPs were likely to be linked with GPs no longer recommending blood glucose monitoring, a previous trigger for the referral of people with diabetes to a CDE.

My practice here in Adelaide has experienced a significant drop-off in referrals, with the data confirming this. I suspect in addition to the issues already outlined, our numbers here have been impacted by the devolution of many CDEs from the State’s tertiary hospitals to community based intermediate care services, which are free to use. Despite that, we are in no way seeing the majority of people with diabetes so room to grow referrals in the future if more people with diabetes requested referrals in their annual plans.
The national numbers will also be influenced by the number of CDEs providing Medicare reimbursed services within each state and territory. This endangered model of care has suffered from a lack of objective review to understand its nuances, including the basics like how many full-time equivalent positions make up this section of the CDE workforce.
Equally the inclusion of these services in pathways of care have also been ignored. It is easier for private practice CDEs to create new models of care or specialised services that others could refer into for targeted input. I have developed a bulk billed service for people with intellectual or developmental disability (IDD) but fail to fill my clinic sessions from a lack of referrals, despite the high level of need for this service. CDEs don’t refer to each other like our medical colleagues are used to doing.
Now, don’t get me wrong, I’m not writing this as a ‘woe is me’ blog … although given the $5/hour I’m earning for my bulk billed sessions one could forgive me if I was… No, I’m writing to focus attention on the need to act as the numbers don’t lie … private practice is on the endangered list as an option for CDEs.
I will even get the ball rolling with a bit of a brainstorm on actions we could take to turn things around …
- ADEA takes a targeted look at private practice with a comprehensive review that asks the right questions to get a full picture of issues, challenges and opportunities
- A NDSS project focussed on strengthening the private practice model of care, increasing GP understanding of the ways CDEs can help them in diabetes management, resources to support strong relationships between CDEs and primary care nurses.
- We give people with diabetes the chance to find out more about the support CDEs can provide with a ADEA/Diabetes Australia campaign, ‘Who’s YOUR CDE?’
- NDSS project to review private practice workforce data and model of care to identify and address the challenges and opportunities with resources to support the role, practitioners and business planning.
- Increase the understanding of general practitioners and people with diabetes on the benefits of structured blood glucose monitoring in understanding a person’s unique version of their condition and problem solving for improved levels.
- ADEA and APNA work together to highlight the complimentary nature of the role of nurses in general practice and their local CDEs
- CDEs in private practice to consider how to create specialised services that address specific needs and encourage referral between CDEs.
- Encourage CDEs to consider private practice as a way to step-down to retirement.
If we do nothing, the data I pull next year from the Medicare site is likely to once again show a continued drop in CDE session numbers. Action is required now, to get private practice into better shape and off the endangered list.